



- Anatomy
- Back pain (dorsalgia)
- Ankylosing spondylitis and other autoimmune diseases
- Headaches
- Warping (deformation) of the spine
- Hernia
- Treatment in Israel
- Diseases of the muscles and ligaments
- Pathology of the soft tissues of the back
- Neurological symptoms and syndromes
- X-ray and other instrumental methods of diagnosis
- Tumors of the spine and spinal cord
- Osteoporosis, osteopenia
- Osteochondrosis
- The answers to the questions of the visitors
- Pathology of the spinal cord
- Diseases of joints and bone tissue of the vertebrae
- Goods
- Spine injury and back
- Methods of treatment of diseases of the spine
Related Posts









How is the reduction of the coccyx in place
Sometimes there are situations related to the traumatic effects that require medical procedure called a reduction of the coccyx.
Tailbone Injury, which causes its displacement relative to the previous position, can be divided into dislocations/subluxations with rupture of the Sacro-coccygeal ligament, or without it, as well as fractures and dislocation.

Dislocation of the coccyx accompanied by displacement of the articular surfaces of the Sacro-coccygeal joint, relative to each other, when subluxation (incomplete dislocation) violation of partial congruence. Luxation/subluxation can be anterior to (e.g., after a heavy fall on the gluteal region) and posterior (e.g., after childbirth). When this damage possible rupture or sprain of the Sacro-coccygeal ligaments strengthen the Sacro-coccygeal joint. Treatment of fresh dislocation/subluxation includes the following activities:
- analgesia
- manipulation to reposition dislocation;
- the appointment of bed rest/gentle treatment during the week;
- NSAIDs and other analgesics;
- physiotherapy
- exercise therapy.
Closed fractures of coccyx and dislocation are much less common than dislocations and subluxations, and are more characteristic of elderly people. The difference in clinical picture of fracture of dislocation of the coccyx is that when fracture occurs, the displacement of fragments (usually anteriorly, sometimes anteriorly and laterally, i.e. To the side). Treatment of fresh fractures includes:
- adequate analgesia;
- manipulation with the aim "to put the fragments in place"
- bed rest for 2-3 weeks with the restoration of health by the end of two months from the time of injury;
- NSAIDs and other analgesics;
- physiotherapy
- exercise therapy.
Technique reposition coccyx dislocation when it is
Directly in front of the reposition the victim should receive adequate analgesia, because the front surface of the sacrum and the tailbone located anatomically near the coccygeal nerve plexus and the fresh trauma the patient experiences severe pain, sometimes torn and can't take some gentle posture. Anesthesia is performed by procaine (or Novocain in combination with lidocaine or alcohol for prolonging the effect) blockade.
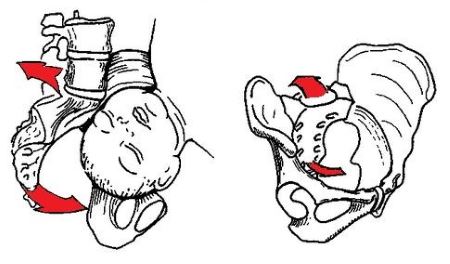
To conduct the anesthesia victim is placed in position on the right side, the feet should be given to the stomach. Also you can position like in the figure below. After anesthesia skin and subcutaneous fat is under control of the index finger introduced into the rectum, between the coccyx and the anus needle first through the dense muscle mass, then in adrectal cellular tissue. The depth of insertion of the needle is about 8 cm of the anesthetic solution is 100-120 ml.

figure 1 – Novocaine blockade used in trauma sacral-coccygeal region (number 2).
After anesthesia of the victim is placed on his stomach, then with the index finger of the right hand through the rectum and the fingers of the left hand from the coccygeal region, carefully creating pressure, trying to straighten out the coccyx. Produced after x-ray control.
The Reduction of the bone fragments in fresh fractures is performed in a similar manner, a course of manipulation similar to that described above.
Why it is impossible to carry out the procedure independently
- for acute trauma to the coccyx the victim has a strong enough pain to make manipulation (editing) without anesthesia.
- it is Impossible to put the fragments in place or to reduce a dislocation without the participation of both hands, that alone could not be implemented.
- When you attempt to reposition the coccyx in the case of dislocations can further damage the sacrococcygeal ligament, healing and regeneration which will be slow. Subsequently may develop coccygodynia.
- When you attempt to match fragments at fracture (back) sharp edge is a high probability of damage to the rectal wall, which can lead to infection of the pararectal cellular tissue, the formation of abscess, sinus tracts.
- According to the degree of pain intensity is impossible to determine what kind of trauma to the sacrococcygeal region causes pain: there are no specific complaints that were specific to the injury of the coccyx, dislocation and/or fracture-only.
- After you perform the manipulation to reposition dislocation or repositioning of bone fragments is definitely a trauma surgeon x-ray control, after independent manipulation is not performed. Therefore, you cannot say about any self-control after reduction or matching of fragments, healing may go wrong, which often leads to the development of coccygodynia.
Tactics correct when stale injuries
Stale injury of the sacrococcygeal region (after 6 months. And more from the moment of traumatic exposure) and the doctors are trying toconservatively, when expressed pain syndrome appointed anti-inflammatories and analgesics, Central muscle relaxants ("Comparison", "Sirdalud"), possibly holding novocaine blockades, and blockades, hydrocortisone (or other corticosteroids).
Reduction of long-standing luxation/subluxation is not made due to the fact that ligaments strengthen the Sacro-coccygeal articulation, spaced out and unable to keep the joint surfaces in normal relation, but to freeze them at a certain period of time is impossible anatomically. Besides, when you try to correct chronic dislocation of the possible further damage to the ligaments of the Sacro-coccygeal joint and the occurrence of pain. Stale fracture of the coccyx is also conservative for the following reasons:
- the Formation of callus over, so the fusion of fragments is already a fait accompli.
- If fusion has not occurred, we developed a "false joint", so it is easier to perform resection (coccygectomy) than to straighten and match fragments.
In the absence of effect from conservative treatment of patient with chronic injuries to the sacrococcygeal region and expressed pain with impaired quality of life recommended the implementation of coccygectomy (resection of the coccyx).